





Introduction
A climate-friendly health system is a health system that both reduces its contribution to climate change and adapts to protect health from climate impacts. In simpler terms, it’s about making healthcare sustainable and resilient in the face of climate change. It is based on low carbon policies, it is climate-proof, it is equitable and health-promoting.
A climate-proof health system combines structural, non-structural, and operational measures to withstand and recover from environmental crises caused by extreme climatic events. Structural solutions include - for example - adapting critical equipment and entire buildings, and using appropriate materials. Non-structural and operational strategies involve robust preparedness plans, early warning systems, coordination with local authorities, and ensuring resilient infrastructure for essential services like power, water, and communication.
There is an extensive literature on climate friendly systems, with several recent developments for health systems. In fact, the increasing welfare and increasing complexity of health procedures triggers a corresponding increase of related carbon emissions. Moreover, the recent occurrence of climatic disasters highlighted that modern health systems are not always resilient against climatic extremes.
We present here below a synthesis of recent report on climate friendly health systems and climate proof health systems.
Figure 1. Interplay between human and planetary health. From UK Health Alliance on Climate Change (2023).
Climate friendly health systems
We present here an extract from the report "Green Surgery", a joint project by the UK Health Alliance on Climate Change, Brighton and Sussex Medical School, and the Centre for Sustainable Healthcare. It provides recommendations to reduce the environmental impact of surgical care. The report identifies single-use items, energy consumption, and anaesthetic gases as major sources of emissions and suggests applying circular economy principles, optimizing energy use in operating theatres, and switching to lower-impact anaesthetics. It offers practical guidance for surgical teams, hospitals, and policymakers to decrease surgery's carbon footprint.
The report emphasises that surgery is energy-intensive, with operating rooms taking a significant part of the power consumption of the hospital. Alongside the importance of using renewable sources of energy, avoiding unnecessary energy use will save both financial resources and emissions. More than 90% of operating room energy consumption relates to heating, ventilation, and air conditioning (HVAC) systems. One case study showed that switching HVAC off at night when theatres were not in use saved 15–36 tonnes of carbon dioxide equivalent (CO2e) and about 30 Keuro per theatre per year. At the national UK scale, this could save some 90 millions of euro and 108,000 tonnes of CO2e annually (Figure 2).
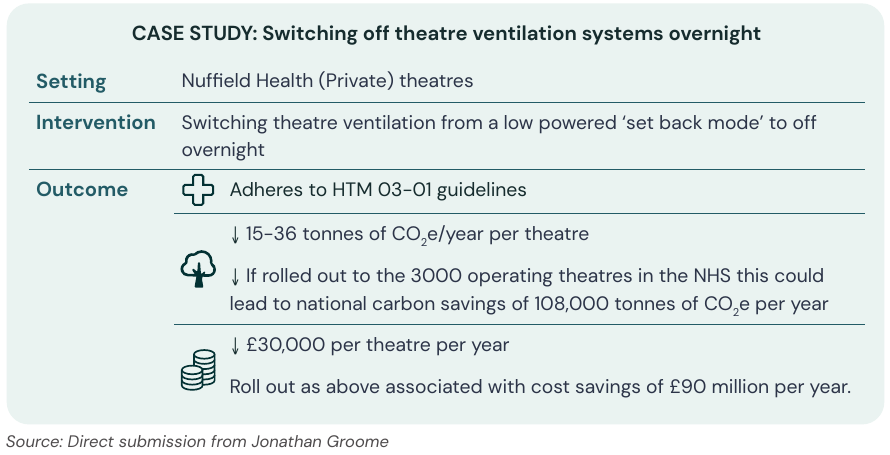
Figure 2. Switching off theatre ventilation contributes to NHS resilience. From UK Health Alliance on Climate Change (2023).
Figure 3 gives an overview of the spending for different surgery types relative to the England annual spend for 2019/20. Obstetrics and gynecology, general surgery, trauma and orthopedics emerge as the most demanding operation sectors.
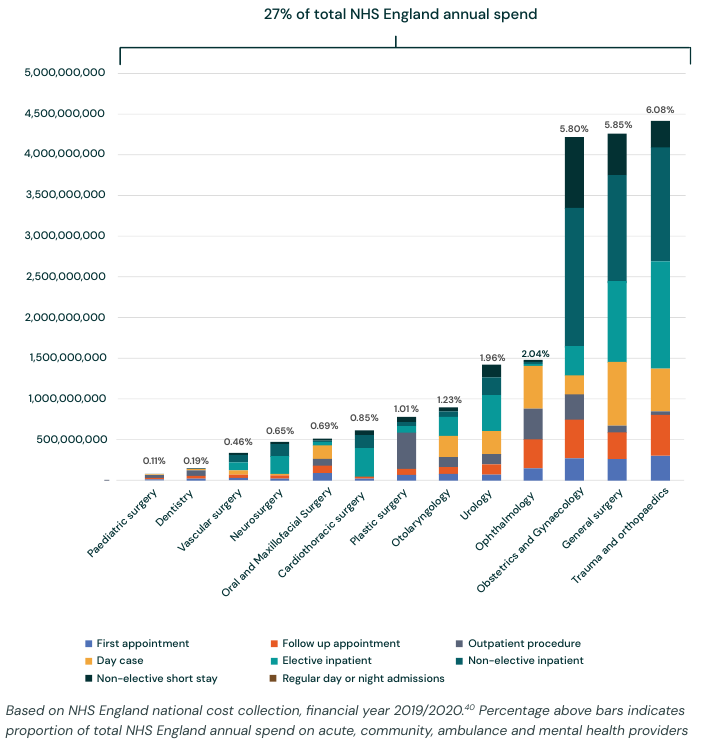
Figure 3. Annual spend on surgical care in the National Health System (NHS) of England, 2019/20. From Figure 2 in UK Health Alliance on Climate Change (2023).
It's also remarkable the report's note that two-thirds of the carbon emissions of some operations are due to single-use surgical products such as operating instruments, gowns, and drapes. Case studies demonstrate that switching to reusable surgical items can save money, reduce carbon, and protect the supply chain from global shocks.
The report also highlights the importance of treatment procedures. A case study at Southampton Hospital reports that there is evidence that ‘early mobilisation’ from 48 hours after admission to intensive care is well tolerated, helps reduce muscle wasting, is a powerful psychological motivator and shortens intensive care and hospital stay, thus implying a significant saving of healthcare resources. In detail, 238 patients were recruited to the early mobilisation programme (EMP) over 24 months. The clinical outcomes show that early mobilisation reduced ventilation days by a mean of 4 days and reduced cardiac intensive care stay by a mean of 6 days in patients after cardiac surgery. This effect was sustained at 12 months and 24 months of the programme. This suggests that the intervention may prevent deconditioning and critical care acquired weakness.
The report identifies the pillars of a sustainable and resilient health system as:
- Reducing need for surgical care;
- Efficient surgical care pathways;
- Operating theatre energy and design;
- Anaesthesia;
- Products used in surgical care;
- Reducing barriers to implementation.
Details on each of the above pillars are given in the report. We present here below a brief focus on operating theatre energy and design, and anesthesia.
Ingredients of an energy efficient operating theatre
Energy use makes up 10% of the NHS carbon emissions footprint. Furthermore, energy prices are raising, therefore triggering a chain of increased use of resources. Designing an energy efficient operating theatre is therefore a key step for moving forward to resilient healthcare (Figure 4).
End-use data suggests that operating theatres are one of the most energy intensive areas of hospitals, using three to six times more energy than clinical wards. The majority (90-99%) of operating theatre energy consumption relates to theatre maintenance (heating, ventilation and air conditioning), whilst the contribution from plug-loads and lighting is estimated at 1.5%-8.4%. Another study found nearly half the energy use was to power the theatre ventilation.
The key points highlighted by UK Health Alliance on Climate Change (2023) are:
- Operating theatres are 3-6 times more energy intensive than clinical wards.
- The majority of theatre energy consumption relates to theatre maintenance (heating, ventilation, and air conditioning).
- There are three main types of ventilation systems: turbulent mixed airflow (least energy), temperature controlled airflow, laminar air flow (most energy).
- Shutdown checklists can be used to prompt staff to switch off theatre equipment out of hours and should be accompanied by turn-on checklists and safety protocols to ensure items are on when required.
- There are opportunities at the stage of theatre design (or retrofit) for installation of motion sensors to control lights, temperature, and ventilation, alongside energy efficient appliances and machinery, and automatic/pedal-controlled taps for surgical scrub.
- At the hospital level, contracts should be drawn with providers of renewable electricity, and installation of combined heat and power facilities.
- There are opportunities across the hospital for installing LED lighting and improving insulation.
Figure 4. Triple bottom line of sustainability. From UK Health Alliance on Climate Change (2023).
Climate friendly anesthesia
Since the recognition that inhaled anesthetics act as powerful greenhouse gases (GHGs), the field of anesthesia has been working to reduce their environmental impact. Efforts include developing low-emission alternatives and improving the efficiency of current agents. Key opportunities for improvement involve: limiting the use of inhaled anesthetics by appropriately opting for total intravenous anesthesia, local, or regional anesthesia as the first choice—using reusable medical equipment whenever it is clinically safe and practical, and cutting down on waste generation. Surgeons also play an important role in minimising the environmental footprint of perioperative care by identifying key areas of high impact and supporting the adoption of more sustainable anesthesia practices. Figure 5 shows a summary of the benefits attainable with local anesthesia.
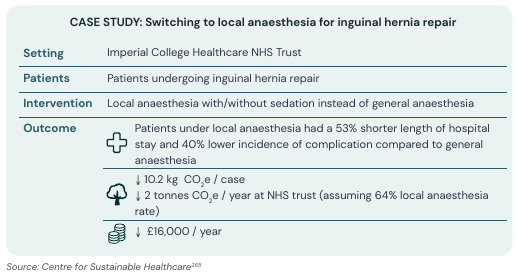
Figure 5. Case study of use of local anesthesia. From UK Health Alliance on Climate Change (2023).
The key points highlighted by UK Health Alliance on Climate Change (2023) are:
- Local, regional, and intravenous anaesthetic techniques may be associated with lower carbon footprint, compared with inhaled anaesthetics.
- Where inhaled anaesthetics are used, sevoflurane followed by isoflurane hold lowest global warming potential, and environmental impact can be further reduced through minimising fresh gas flows.
- Desflurane should not be used, bar exceptional circumstances.
- Nitrous oxide is another powerful greenhouse gas, and emissions can be minimised through non-pharmacological methods to manage patient anxiety, decommissioning of centrally piped nitrous oxide (and substitution by portable cylinders), and nitrous oxide cracking technologies.
- Pharmaceutical wastage can be reduced through only opening what is needed; all pharmaceutical waste should be disposed of appropriately.
- There is currently a lack of robust evidence on capture rates of volatile capture technologies for anaesthetic gas waste.
We suggest to look at the other pillars for a resilient National Healthcare System in the report of the UK Health Alliance on Climate Change (2023).
Climate proof health systems
From Montanari et al. (2024) one reads:
In July 2021 heavy and widespread rainfall caused catastrophic flooding in parts of Germany, Belgium, Luxembourg and the Netherlands with 221 fatalities and EUR 46 billion economic damage (Munich Re, 2022). A total of 134 people died alone along the river Ahr in Germany, a tributary of the Rhine with a catchment area of less than 900 km<sup>2</sup>. Although a precise rainfall forecast was only possible with a lead time of a few hours, the potential for extraordinary rainfall was provided at least 2 d in advance (Mohr et al., 2023). Nevertheless, this flood took both people and disaster management by surprise. The severity of the flooding was underestimated, the state of emergency was declared too late and evacuations were not initiated in time (Thieken et al., 2023), although the specific circumstances of the warning and disaster management are still under investigation by inquiry commissions (Landtag RLP, 2023). The first fatalities in the Ahr catchment occurred in the late afternoon of 14 July in Dorsel in the upstream Ahr catchment. The flood wave took around 7 h to travel downstream, and at 02:00 the next day 12 people in a facility for mentally and physically handicapped were trapped and drowned in Sinzig, 60 km downstream of Dorsel. In many regions, the inundation extent of July 2021 exceeded the flood scenarios of the official flood maps by far.
During the 2021 flood in Germany, hospitals suffered from power shutdown while water was invading the rooms, and the patients had to be carried out by hands, walking down along the stairs.
In May 2023, the Emilia-Romagna region of Italy—particularly the Romagna area—experienced catastrophic floods following intense rainfall, forcing the evacuation of more than 36,000 people and disrupting essential services. The regional health system, led by Azienda USL della Romagna - in coordination with the civil protection authorities - rapidly activated its emergency operations. Early assessments identified vulnerable groups such as the elderly, disabled, and chronically ill, who were relocated to protected facilities and community shelters. Hygiene inspections and infection-control protocols were immediately deployed to prevent outbreaks, while the Local Health Authority distributed guidance leaflets on wound protection, safe cleanup, and avoiding contact with contaminated water. Targeted vaccination campaigns were launched against tetanus and hepatitis A, and syndromic surveillance systems monitored gastrointestinal, trauma, and mental-health cases emerging from affected populations.
Hospitals and primary-care clinics continued to function despite widespread infrastructural damage, thanks to contingency plans, mobile health units, and volunteer coordination. Emergency departments reported higher-severity cases, mainly trauma and mental distress, though overall service continuity was maintained through strong integration between public health, primary care, and social services. The health system’s communication teams worked closely with municipalities to issue daily risk updates and hygiene recommendations, while environmental health units monitored water quality and vector-borne disease risks. In the aftermath, attention shifted to long-term recovery—psychological support, restoration of home-care visits, and resumption of routine check-ups for chronic patients. The 2023 Romagna floods ultimately highlighted both the strengths of Italy’s decentralized, community-based healthcare model and critical gaps in data integration, volunteer coordination, and disaster planning—offering key lessons for building a more flood-resilient health system in the era of climate change. For more details see Valente et al. (2023).
Quoting from "Preparing health systems for shocks - Japan's experience of enhancing the resilience of its health system":
In terms of the impact of floods on health facilities, during the 2018 heavy rains that caused river flooding and landslides impacting more than 10 prefectures in southwestern Japan, approximately 95 medical facilities were affected by flooding, power outages and water service disruptions at their hospitals and clinics. In Mabi District, Kurashiki City, Okayama Prefecture, one of the most devastated areas due to a levee break that led to more than 50 deaths, the Mabi Memorial Hospital was inundated up to its first floor ceiling. More than 300 patients and workers were temporarily trapped within the hospital building unable to access lifeline infrastructure services. However, thanks to the quick rescue and emergency transport efforts provided by the Self Defense Force, Fire and Disaster Management Agency (FDMA), and DMAT, there were no casualties during that temporary period of isolation. Lifeline infrastructure in Mabi City was eventually restored, including power within five days, water supply within two weeks, and medical services within 10 days (resumed provisionally from vehicles). [...] this flood event in Mabi encouraged other hospital and wide stakeholder groups in the region to invest in and improve the resilience of their facilities and Business Continuity Plan for the region.
The bigger picture and the pillars for a resilient health system resulting from the Japanese experience are depicted in Figures 6 and 7.
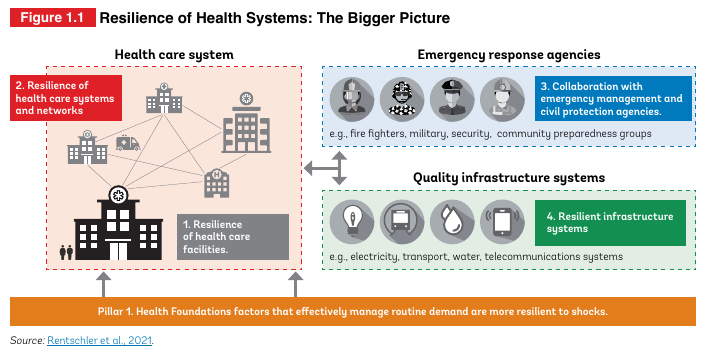
Figure 6. Resilience of Health Systems: The Bigger Picture resulting from the Japanese experience. From "Preparing health systems for shocks - Japan's experience of enhancing the resilience of its health system"
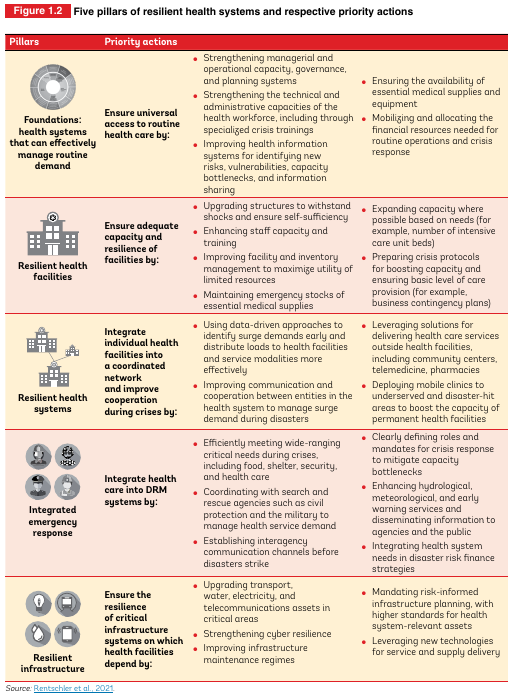
Figure 7. Five pillars of resilient health systems and respective priority actions resulting from the Japanese experience. From "Preparing health systems for shocks - Japan's experience of enhancing the resilience of its health system"
The above three examples highlight the value of preparedness in the health system. Sometimes extreme climatic events are deemed to be impossible, therefore causing lack of resilience.
What can we do to make the health care system in general, and hospitals in particular, climate proof? We will focus here below on the case of flooding.
Flood proof health systems
Flood-proofing health systems means ensuring that healthcare services remain functional, accessible, and safe during and after flooding events. This involves infrastructure resilience, preparedness planning, and community coordination. Some key strategies:
Infrastructure and Facility Design
Flood mapping: through hydraulic models, get a map of water depth and water flow velocity that may occur during a flood;
Elevate critical areas: Place generators, laboratories, pharmacies, and patient wards above known flood levels.
Flood-resistant construction: Use waterproof materials, sealed walls, raised foundations, and flood barriers.
Drainage and landscaping: Install effective stormwater drainage systems and use permeable pavements to reduce runoff.
Backup utilities: Ensure backup power (elevated generators, solar systems) and independent water supply.
Relocation or redundancy: Build backup facilities outside flood-prone zones for essential services (e.g., regional storage for vaccines or medicines).
Preparedness and Emergency Planning
Continuity of operations plans (COOP): Include evacuation routes, communication systems, and essential service prioritization.
Emergency supplies and stockpiling: Store essential medicines, water purification tools, and emergency kits in waterproof containers.
Training and drills: Regularly train health workers on flood response, triage in flooded conditions, and safe facility evacuation.
Coordination networks: Establish links with local disaster management agencies, NGOs, and emergency responders.
Service Delivery and Health System Resilience
Decentralize services: Enable community-level care and mobile health units for when main hospitals are inaccessible.
Digital health systems: Use telemedicine and cloud-based patient records that remain accessible off-site.
Rapid response teams: Deploy trained health professionals for emergency outreach in flood-affected areas.
Cold chain protection: Use portable, solar-powered vaccine refrigerators and temperature monitoring devices.
Environmental and Community-Based Strategies
Community education: Promote public awareness on hygiene, water safety, and flood-related disease prevention (e.g., leptospirosis, cholera).
Safe water and sanitation systems: Protect wells, install elevated latrines, and distribute water purification materials.
Health Workforce
Training and drills: PHC staff need training in flood-response protocols (evacuation, safe patient transfer, continuity of essential services under water-loss/power-loss conditions). A Saudi Arabia study found that although willingness was high, competencies/guidelines were missing.
Role flexibility and task-shifting: In flood conditions, usual referral/hospital services may be disrupted — PHC staff may need to handle expanded roles (first aid, triage, outreach). The integration of emergency care into PHC was discussed in LMICs literature.
Staff safety and retention: Ensure staff can reach the facility despite floods (transport arrangements), that living/working conditions remain safe, and that psychosocial support is available (floods impose trauma on staff too).
There are several success stories at the international that may inspire a global strategy. For instance, in Japan the above mentioned report Preparing health systems for shocks - Japan's experience of enhancing the resilience of its health system presents the interesting case study described in Figure 8 where a hospital was flood proofed.

Figure 8. Case study. Example of flood protection measures at Kurashiki Central Hospital. From "Preparing health systems for shocks - Japan's experience of enhancing the resilience of its health system"
Another relevant example is offered by Cambodia where flood shelters were recently made available. Indeed, flooding is by far the most common and frequent natural hazard facing Cambodia, a threat to lives and livelihoods across the country. Climate change will likely further increase the frequency of severe flood events. In 2011, a flood affected more than 1,700,000 people, killed 250, and left 50,000 families homeless.
Despite the high flood risk, Cambodia has only nine multi-purpose flood shelters, serving approximately 12,000 people. According to conservative estimates based on GFDRR analysis, more than 3 million people are exposed to significant flood risks, with a 10 percent probability per decade of them experiencing floods exceeding 1.5 meters in depth. Projections from this analysis indicate that the number of people exposed could rise to nearly 8 million by 2050. Limited shelter capacity regularly forces many Cambodians to seek refuge in temporary shelters, which lack basic safety, water and sanitation; medical aid; and appropriate spaces for vulnerable groups such as women, children, and elderly adults.
Against this backdrop, Cambodia has prioritized the construction of multi-purpose flood shelters to protect the most vulnerable populations, as part of efforts to protect lives and livelihoods against the intensifying flood risk. Drawing on GFDRR’s expertise at the intersection of climate risk management, disaster risk management (DRM), and health, the facility has helped Cambodia ensure that the shelters not only provide the maximum protection, but also fill gaps in health care service delivery during non-emergency times. This support has been provided through the Japan-World Bank Program for Mainstreaming Disaster Risk Management in Developing Countries.
Another relevant example is given by the UK Health Security Agency who presented the guidance Flood-health action card for health and social care providers. It is an interesting set of guidelines to support all year round flood preparedness, pre-emergency management (before flooding), emergency management (during flooding), flood recovery (after flooding).
Conclusions
The strength of a health system is truly tested not in times of calm, but in moments of crisis. Preparedness is not a luxury — it is a necessity that saves lives, preserves stability, and ensures that communities can recover with dignity. Building resilient health systems requires more than emergency response plans; it demands sustained investment in infrastructure, workforce training, data systems, and community engagement.
As we have seen, integrating disaster risk reduction into every layer of health governance — from hospitals to national policy — transforms reactive systems into proactive ones. A shared commitment is needed: to make preparedness a core value of our health systems, so that when calamities strike, our response is swift, coordinated, and efficient.
References
Brighton & Sussex Medical School, Centre for Sustainable Healthcare, and UK Health Alliance on Climate Change (2023). Green surgery: Reducing the environmental impact of surgical care (v1.1). London: UKHACC. https://ukhealthalliance.org/sustainable-healthcare/green-surgery-report/
Montanari, A., Merz, B., & Blöschl, G. (2024). HESS Opinions: The sword of Damocles of the impossible flood. Hydrology and Earth System Sciences, 28(12), 2603-2615.
Valente, M., Zanellati, M., Facci, G., Zanna, N., Petrone, E., Moretti, E., ... & Ragazzoni, L. (2023). Health system response to the 2023 floods in Emilia-Romagna, Italy: a field report. Prehospital and disaster medicine, 38(6), 813-817.
Download the powerpoint presentation of this lecture
Last modified on November 13, 2025
- 128 views